When Primary Care Meets Passwords
Reflections on Digitalization at the Frontline of Public Primary Care by Vikash R. Keshri

Welcome to Thinking Health System. This newsletter is where I share reflections from the field, ideas from health policy and systems research, and conversations about how health systems actually work, not just how we expect them to.
Health systems are constantly changing and evolving, and are therefore learning entities. At the frontline of India’s public health system is the Health Sub-Centre (HSC), most of which have now been upgraded to Health and Wellness Centres (HWCs) and rechristened as Ayushman Arogya Mandirs (AAMs), although HWC remains the more familiar and widely used term.
For years, an HSC was staffed by one or two Auxiliary Nurse Midwives (ANMs) and a Male Health Worker (HW). Together, they primarily provided maternal and child healthcare and managed common ailments. With the upgradation of HSCs into HWCs, a new cadre of mid-level health providers, called Community Health Officers (CHOs), was introduced to deliver Comprehensive Primary Health Care (CPHC). The introduction of CHOs is one of the most significant changes at the frontline of public primary care in India. They are young professionals, qualified either in nursing or in Indian systems of medicine, and trained to provide the 12 packages of CPHC, including care for non-communicable diseases and common emergencies. Obviously, the expectations placed on a single CHO are enormous.


The HWC team, comprising the CHO, ANM and Male Health Worker, is also responsible for outreach activities in villages within its catchment area. They organise regular Village Health and Nutrition Days, where they deliver essential primary healthcare services. It is therefore safe to say that a well-functioning HWC is the backbone of India’s public health system.
Then enter the devices: a mobile phone, tablet, and/or computer, and the effort to digitalise public health systems and their processes.
Over the years, during my visits to HWCs and interactions with CHOs, ANMs and Health Workers, I have often sensed their frustration with the growing burden of digitalization and the disproportionate workload it places on them. This feeling was reinforced during a recent learning visit.
I visited a well-functioning HWC in a peri-urban area led by a highly qualified CHO, recognized nationally as a champion of public health. I also met, probably for the first time, a male ANM (I have met many male nurses before, but this was my first interaction with someone trained specifically as an ANM).
At first glance, the centre appeared to be functioning exceptionally well. The CHO managed a busy outpatient clinic with around 30 patients a day, most of whom returned for follow-up care for non-communicable diseases.
But what immediately caught my attention was a register containing usernames, and login details for numerous digital platforms that the health workers were expected to update regularly.
During our interaction, the staff listed an astonishing number of portals and applications requiring routine data entry. These included:
JANANI (Journey of Antenatal, Natal and Neonatal Integrated Care), formerly the RCH Portal
NCD screening and follow-up portals
U-WIN immunization platform
Nikshay for tuberculosis
Family Planning Logistics Management Information System (FPLMIS)
Integrated Health Information Platform (IHIP/IDSP)
Ayushman Bharat–Health and Wellness Centre portal
eSanjeevani teleconsultation platform
Drug and vaccine inventory management systems
State diagnostic portals
Performance dashboards and key performance indicators (NQAS)
Programme-specific Google Sheets for high-risk pregnancy and rabies monitoring
Cough AI
Performance Linked Payment (PLP) data entry
Cold chain management
Other programme-specific reporting requirements
Some activities required daily data entry, others weekly updates, while several demanded parallel maintenance of both physical registers and digital portals.
For example, immunisation sessions required updates in U-WIN while maintaining physical records. Janani-related reporting often involved duplicate systems. Tuberculosis patients needed monthly tracking in Nikshay. High-risk pregnancies and rabies cases were additionally monitored through separate Google Sheets.
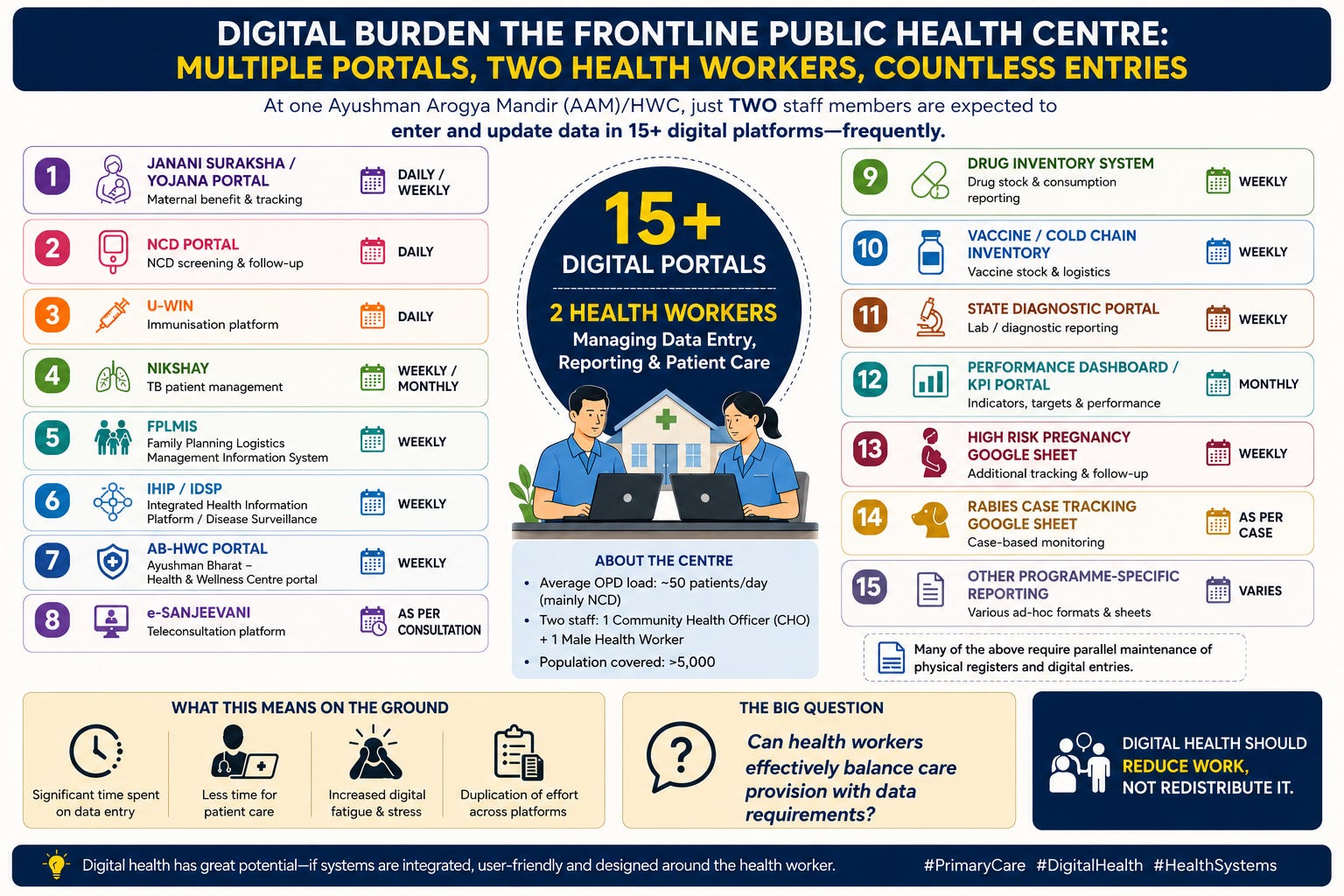
The obvious question that emerged was: How will health workers get time to balance healthcare and data management?
This is not a criticism of digitalization itself. Digital platforms have enormous potential to strengthen continuity of care, improve monitoring, enable population health management and enhance accountability. The problem is fragmentation.
Every public health program has built its own digital solution. From the perspective of a programmme manager sitting at the state or national level, each platform may appear logical and indispensable. But at the facility level, these systems simply accumulate. We have tried to do away with Vertical health programme but we are yet to do away with vertical digital portals. The result is something we rarely measure digital fatigue among frontline health workers.
Primary care workers are increasingly becoming data collectors and data managers, in addition to being healthcare providers and community health workers.
The irony is difficult to ignore. HWCs were envisioned as platforms for comprehensive primary healthcare, places where prevention, health promotion, chronic disease management and community engagement would flourish. Yet, increasingly, a substantial part of a provider’s day is spent moving between logins, portals and spreadsheets, and figuring out passwords. This also raises a larger policy question:
Are we building digital systems for health systems, or designing them vertically around each public health programme?
Because every additional portal comes with an opportunity cost. Every extra data entry takes away a few more minutes from patient counselling, community engagement or clinical care.
Digital health should reduce the work of frontline health workers and not complicate them. As India continues its ambitious digital health journey, perhaps we should ask one simple question before launching another platform: Can a frontline health worker realistically do all this and still remain a healthcare provider?
Disclaimer: views expressed are personal